
Dec 27, 2011
Dec 18, 2011
PAPER OF THE WEEK
Reference Values for Normal Pulmonary Artery Dimensions by Noncontrast
Cardiac Computed Tomography: The Framingham Heart Study
Dr. Truong et al, studied 3171 asymptomatic patients and measured the main pulmonary artery transverse axial diameter. For simplicity, they established 29 mm in men and 27 mm in women as sex specific normative reference values for mPA and 0.9 for ratio PA.
Dec 10, 2011
Dec 5, 2011
Call for Associate Editor, Case of the Week
Call for Associate Editor, Case of the Week:
Interested candidates please send your CV to c.bucciarelli-ducci@rbht.nhs.uk. Interviews will take place during SCMR 2012 meeting. Applications from Asia and South America are particularly encouraged.
Interested candidates please send your CV to c.bucciarelli-ducci@rbht.nhs.uk. Interviews will take place during SCMR 2012 meeting. Applications from Asia and South America are particularly encouraged.
Short term buying

More than half will stay put and not upgrade their machines in the next year.
Juliano
Nov 22, 2011
Paper of the Week
Myocardial infarction in women with normal coronaries: use of CMR
Circulation. 2011; 124: 1414-1425
Myocardial infarction with apparent normal epicardial arteries occurs in a specific number of cases especially in women. Dr Reynolds and cols analyzed 50 women with documented increase in troponin and invasive angiography plus IVUS with < 50% stenosis. An abnormal CMR was found in 59% of these women with LGE present in 34% and edema (by T2W imaging) in 18%. Interestingly, edema was correlated with myocardial segments irrigated by a coronary with plaque disruption. The most common pattern of LGE was transmural or subendocardial (10/17 - 59%) but mixed and purely nonischemic patterns were also rather frequent (41%). The authors conclude that the use of IVUS and especially of CMR can aid in the identification of the causes underlying such clinical situations with possible therapeutical consequences.
Circulation. 2011; 124: 1414-1425
Myocardial infarction with apparent normal epicardial arteries occurs in a specific number of cases especially in women. Dr Reynolds and cols analyzed 50 women with documented increase in troponin and invasive angiography plus IVUS with < 50% stenosis. An abnormal CMR was found in 59% of these women with LGE present in 34% and edema (by T2W imaging) in 18%. Interestingly, edema was correlated with myocardial segments irrigated by a coronary with plaque disruption. The most common pattern of LGE was transmural or subendocardial (10/17 - 59%) but mixed and purely nonischemic patterns were also rather frequent (41%). The authors conclude that the use of IVUS and especially of CMR can aid in the identification of the causes underlying such clinical situations with possible therapeutical consequences.
Nov 19, 2011
Nov 11, 2011
Atlas CMR internacional
Divulgando:
CAP case upload site - OPEN
Unread postby ayoung348 » Thu Nov 10, 2011 9:17 pm
The Cardiac Atlas Project case upload site is now open. This research project is endorsed by SCMR and aims to provide atlas-based CMR analysis tools for the community. Check it out at http://www.scmr.org/Research/cap-dicom-transfer.html. I'll also start a forum thread called "Cardiac Atlas Project"
Regards
Alistair
CAP case upload site - OPEN
Unread postby ayoung348 » Thu Nov 10, 2011 9:17 pm
The Cardiac Atlas Project case upload site is now open. This research project is endorsed by SCMR and aims to provide atlas-based CMR analysis tools for the community. Check it out at http://www.scmr.org/Research/cap-dicom-transfer.html. I'll also start a forum thread called "Cardiac Atlas Project"
Regards
Alistair
Nov 1, 2011

Oct 22, 2011
Paper of the Week
Incremental Prognostic Significance of Combined Cardiac Magnetic Resonance
Imaging, Adenosine Stress Perfusion, Delayed Enhancement, and Left Ventricular Function Over Preimaging Information for the Prediction of Adverse Events
(Circulation. 2011;123:1509-1518.)
Dr Bingham and cols followed up 908 consecutive patients who underwent combined CMR for suspicion of coronary stenosis and/or ischemia at 2.6_1.2 years, during which 101 total cardiac events occurred (all-cause death, myocardial infarction, or late revascularization). In the studied population, cardiac magnetic resonance imaging without abnormalities had a 2.4% event rate per year (<1% cardiac death or myocardial infarction). Abnormal CMR was associated with event rates of 5.6% to 7.0% per year, varying with which and how many components were abnormal. They concluded that CMR analysis of ventricular volume, aortic flow, myocardial viability, and stress perfusion all add incremental value for prediction of adverse events over pre-CMR data and can be combined to further enhance prognostication. Normal combined CMR confers a low risk of subsequent cardiac events.
Oct 16, 2011
Paper of the Week
Role of Cardiovascular Magnetic Resonance as a Gatekeeper to Invasive Coronary Angiography in Patients Presenting With Heart Failure of Unknown Etiology. (Circulation. 2011;124:1351-1360.)
Dr. Assomull and cols assessed the diagnostic accuracy of a cardiovascular magnetic resonance (CMR) protocol incorporating late gadolinium enhancement (LGE) and magnetic resonance coronary angiography (CA) as a noninvasive gatekeeper to CA in determining the etiology of heart failure in patients and concluded that LGE-CMR is a safe, clinically effective, and potentially economical gatekeeper to CA in patients presenting with heart failure of uncertain etiology.
Oct 6, 2011
PAPER OF THE WEEK
Prevalence of scarred and dysfunctional myocardium in patients with heart failure of ischaemic origin: A cardiovascular magnetic resonance study
Journal of Cardiovascular Magnetic Resonance 2011, 13:53
Dr. Christos V Bourantas and cols assessed the prevalence of dysfunctional myocardium, including partial thickness scar in patients with heart failure and ischaemic heart disease who denied angina symptoms. They concluded that in their cohort of patients with left ventricular systolic dysfunction and ischaemic heart disease, about half of all segments had contractile dysfunction but only one third of these had >50% of the wall thickness affected by scar, suggesting that most dysfunctional segments could improve in response to an appropriate intervention.
Journal of Cardiovascular Magnetic Resonance 2011, 13:53
Dr. Christos V Bourantas and cols assessed the prevalence of dysfunctional myocardium, including partial thickness scar in patients with heart failure and ischaemic heart disease who denied angina symptoms. They concluded that in their cohort of patients with left ventricular systolic dysfunction and ischaemic heart disease, about half of all segments had contractile dysfunction but only one third of these had >50% of the wall thickness affected by scar, suggesting that most dysfunctional segments could improve in response to an appropriate intervention.
Sep 25, 2011

Sep 20, 2011
The Association of Pericardial Fat with Coronary Artery Plaque Index at MR Imaging: The Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
Purpose: To determine the relationship of pericardial fat, which secretes proinflammatory markers that have been implicated in coronary atherosclerosis, with atherosclerotic plaque in an asymptomatic population–based cohort.
Materials and Methods: In this institutional review board–approved study, all participants supplied written informed consent. One hundred eighty-three participants (89 women, 94 men; mean age, 61 years ± 9 [standard deviation]) from the community-based Multi-Ethnic Study of Atherosclerosis (MESA) were included. The coronary artery eccentricity (ratio of maximal to minimal coronary artery wall thickness) was determined by using magnetic resonance (MR) imaging and served as an index of plaque burden. The pericardial fat volume was determined by using computed tomography. Linear regression coefficient analysis was used to correlate pericardial fat volume with coronary artery wall thickness and plaque eccentricity.
Results: Pericardial fat volume correlated significantly with degree of plaque eccentricity (P < .05) in both men and women. After adjustments for body mass index (BMI) and waist circumference, traditional risk factors, C-reactive protein level, and coronary artery calcium content, the relationship between pericardial fat and plaque eccentricity remained significant in men (P < .01) but not in women. BMI and waist circumference correlated with degree of plaque eccentricity in the univariate model (P < .05) but not after adjustment for pericardial fat volume or traditional risk factors.
Conclusion: Pericardial fat volume, rather than BMI and waist circumference, was more strongly related to plaque eccentricity as a measure of coronary atherosclerotic plaque burden. The results support the proposed role of pericardial fat in association with atherosclerosis.
© RSNA, 2011
Abstract
Purpose: To determine the relationship of pericardial fat, which secretes proinflammatory markers that have been implicated in coronary atherosclerosis, with atherosclerotic plaque in an asymptomatic population–based cohort.
Materials and Methods: In this institutional review board–approved study, all participants supplied written informed consent. One hundred eighty-three participants (89 women, 94 men; mean age, 61 years ± 9 [standard deviation]) from the community-based Multi-Ethnic Study of Atherosclerosis (MESA) were included. The coronary artery eccentricity (ratio of maximal to minimal coronary artery wall thickness) was determined by using magnetic resonance (MR) imaging and served as an index of plaque burden. The pericardial fat volume was determined by using computed tomography. Linear regression coefficient analysis was used to correlate pericardial fat volume with coronary artery wall thickness and plaque eccentricity.
Results: Pericardial fat volume correlated significantly with degree of plaque eccentricity (P < .05) in both men and women. After adjustments for body mass index (BMI) and waist circumference, traditional risk factors, C-reactive protein level, and coronary artery calcium content, the relationship between pericardial fat and plaque eccentricity remained significant in men (P < .01) but not in women. BMI and waist circumference correlated with degree of plaque eccentricity in the univariate model (P < .05) but not after adjustment for pericardial fat volume or traditional risk factors.
Conclusion: Pericardial fat volume, rather than BMI and waist circumference, was more strongly related to plaque eccentricity as a measure of coronary atherosclerotic plaque burden. The results support the proposed role of pericardial fat in association with atherosclerosis.
© RSNA, 2011
Sep 19, 2011
PAPER OF THE WEEK
On improvement in ejection fraction with Iron Chelation in Thalassemia Major and the risk of future heart failure.
J Cardiovasc Magn Reson. 2011 Sep 12;13(1):45.
Prof. Pennell and his group concluded that during treatment with iron chelators for cardiac siderosis, even small increases in LVEF in TM patients are associated with a significantly reduced risk of the development of heart failure. Thus the iron chelator induced improvements in LVEF of 2.6% to 3.1% that have been observed in randomized controlled trials, are associated with risk reductions of 25.5% to 46.4% for the development of heart failure over 12 months, which is clinically meaningful.
J Cardiovasc Magn Reson. 2011 Sep 12;13(1):45.
Prof. Pennell and his group concluded that during treatment with iron chelators for cardiac siderosis, even small increases in LVEF in TM patients are associated with a significantly reduced risk of the development of heart failure. Thus the iron chelator induced improvements in LVEF of 2.6% to 3.1% that have been observed in randomized controlled trials, are associated with risk reductions of 25.5% to 46.4% for the development of heart failure over 12 months, which is clinically meaningful.
Sep 12, 2011
PAPER OF THE WEEK
Prognostic Value and Determinants of a Hypointense Infarct Core in T2-Weighted Cardiac Magnetic Resonance in Acute Reperfused ST-Elevation–Myocardial Infarction (Circulation: Cardiovascular Imaging. 2011; 4: 354-362 )
Dr. Eitel and cols, evaluated determinants and prognostic impact of a hypointense infarct core in T2-weighted CMR images, studied in patients after acute, reperfused ST-elevation–myocardial infarction and concluded that a hypointense infarct core within the area at risk of reperfused infarcted myocardium in T2-weighted CMR is closely related to infarct size, microvascular obstruction, and impaired left ventricular function, with subsequent adverse clinical outcome.
Dr. Eitel and cols, evaluated determinants and prognostic impact of a hypointense infarct core in T2-weighted CMR images, studied in patients after acute, reperfused ST-elevation–myocardial infarction and concluded that a hypointense infarct core within the area at risk of reperfused infarcted myocardium in T2-weighted CMR is closely related to infarct size, microvascular obstruction, and impaired left ventricular function, with subsequent adverse clinical outcome.
Sep 4, 2011
Study hours

Responders put a lot of hours into studying CMR. Certainly this is one of the reasons the method is keeps growing in Latin America.
Aug 21, 2011
Paper of the Week
Prognostic Value and Determinants of a Hypointense Infarct Core in T2-Weighted Cardiac Magnetic Resonance in Acute Reperfused ST-Elevation–Myocardial Infarction
Circulation: Cardiovascular Imaging. 2011; 4: 354-362
Dr. Eitel and cols evaluated determinants and prognostic impact of a hypointense infarct core in T2-weighted CMR images, studied in patients after acute, reperfused ST-elevation–myocardial infarction. and concluded that it`s is closely related to infarct size, microvascular obstruction, and impaired left ventricular function, with subsequent adverse clinical outcome.
Aug 16, 2011
Aug 8, 2011
PAPER OF THE WEEK
Value of scar imaging and inotropic reserve combination for the prediction of segmental and global left ventricular functional recovery after revascularisation (Journal of Cardiovascular Magnetic Resonance 2011, 13:35)
Dr. Glaveckaite and cols compared three cardiovascular magnetic resonance (CMR) viability parameters: inotropic reserve (IR) during low-dose dobutamine (LDD) administration, late gadolinium enhancement transmurality (LGE) and thickness of the non-contrast-enhanced myocardial rim surrounding the scar (RIM) and concluded that LDD-CMR is superior to LGE-CMR as a predictor of segmental recovery. They show that the advantage is greatest in the segments with an LGE from 26% to 75%. The RIM cut-off value of 4 mm had no superiority over the LGE cut-off value of 50% in predicting the segmental recovery. Patients with [greater than or equal to]50% of viable segments from all dysfunctional and revascularised had a tendency to improve LVEF by [greater than or equal to]5% after revascularisation.
Dr. Glaveckaite and cols compared three cardiovascular magnetic resonance (CMR) viability parameters: inotropic reserve (IR) during low-dose dobutamine (LDD) administration, late gadolinium enhancement transmurality (LGE) and thickness of the non-contrast-enhanced myocardial rim surrounding the scar (RIM) and concluded that LDD-CMR is superior to LGE-CMR as a predictor of segmental recovery. They show that the advantage is greatest in the segments with an LGE from 26% to 75%. The RIM cut-off value of 4 mm had no superiority over the LGE cut-off value of 50% in predicting the segmental recovery. Patients with [greater than or equal to]50% of viable segments from all dysfunctional and revascularised had a tendency to improve LVEF by [greater than or equal to]5% after revascularisation.

Jul 29, 2011

LA CONQUISTA.................
SIN DUDA ALGUNA RM CARDIACA ES FASCINANTE.........A NUESTROS AMIGOS ELECTROFISIOLOGOS PREMIARNOS UNA VEZ MAS........CON EL GRAN APORTE QUE ESTAN RECIBIENDO DE LA IMAGENOLOGIA CARDIACA.
Imaging of Scar in Patients with Ventricular Arrhythmias of Right Ventricular Origin: Cardiac Magnetic Resonance Versus Electroanatomic Mapping.
Santangeli P, Hamilton-Craig C, Russo AD, Pieroni M, Casella M, Pelargonio G, Biase LD, Smaldone C, Bartoletti S, Narducci ML, Tondo C, Bellocci F, Natale A.
Abstract
Imaging of Scar in Patients with RV Origin Arrhythmias: CMR Versus EAM. Introduction: Assessment of late gadolinium enhancement (LGE) at cardiac magnetic resonance is often used to detect scar in patients with arrhythmias of right ventricular (RV) origin. Recently, electroanatomic mapping (EAM) has been shown to reliably detect scars corresponding to different cardiomyopathic substrates. We compared LGE with EAM for the detection of scar in patients with arrhythmias of RV origin.
Methods and Results: Thirty-one patients with RV arrhythmias and biopsy-proven structural heart disease (18 ARVC and 13 myocarditis), and 5 with idiopathic RV outflow tract arrhythmias underwent LGE analysis and EAM with scar validation through EAM-guided endomyocardial biopsy. EAM scars were present in 23 (64%) patients (all with structural heart disease), whereas LGE was present only in 12 (33%). In 2 cases, EAM provided a false-positive diagnosis of a small scar in the basal perivalvular area. LGE correctly diagnosed EAM scar in 48% of patients, resulting in high positive (92%) but low negative (50%) predictive values. The distribution of LGE was significantly associated with the distribution of EAM scars (P < 0.001 in the free wall, P = 0.003 in the outflow tract, and P = 0.023 in the posterior/inferior wall). Presence of LGE reflected a higher extension of EAM scars (34.4 ± 16.5% vs 7.9 ± 10.1% of the RV area, P < 0.001). At receiver operating characteristic (ROC) analysis, an extension of scar ≥20% of the RV area was the best cut-off value to detect LGE (sensitivity 83%, specificity 92%). Of note, LGE missed 10 of 11 (91%) patients with EAM scars <20% of RV area.
Conclusions: LGE is significantly less sensitive than EAM in identifying RV cardiomyopathic substrates. Absence of LGE does not rule out the presence of small scars, and EAM with biopsy should be considered to increase the diagnostic yield. (J Cardiovasc Electrophysiol, Vol. pp. 1-8).
J Cardiovasc Electrophysiol. 2011 Jul 7
Jul 13, 2011
PAPER OF THE WEEK
Effect of Deferiprone or Deferoxamine on Right Ventricular Function in Thalassemia Major Patients with Myocardial Iron Overload (JCMR 2011, 13:34)
Dr. G. Smith from Dr. Pennell's group, studied Thalassaemia major patients and made a retrospective analysis of a prospective randomized controlled trial, concluding that deferiprone monotherapy was superior to deferoxamine for improvement in RV EF and end-systolic volume. This improvement in the RV volumes and function may contribute to the improved cardiac outcomes seen with deferiprone.
Dr. G. Smith from Dr. Pennell's group, studied Thalassaemia major patients and made a retrospective analysis of a prospective randomized controlled trial, concluding that deferiprone monotherapy was superior to deferoxamine for improvement in RV EF and end-systolic volume. This improvement in the RV volumes and function may contribute to the improved cardiac outcomes seen with deferiprone.
Jul 11, 2011
JCMR IF increased

The new JCMR Impact Factor has increased to a solid 4.33. In the last year it has steadily risen with 2010 showing a huge gain:
2006 1.74
2007 1.87
2008 2.15
2009 2.28
2010 4.33
Interestingly, self-reporting has been relatively low at 14% with a bit upward numbers to 26% to years used in IF calculation. Even without self cites, it would still post a significant increase to 3.2 this year.
How do we compare to other CV and Rad journals? The median values for CV and Rad are 1.99 and 1.87 respectively. Here is a selected list of journals in order of IF:
Radiology 6.1
JACC Imaging 5.5
Circ Imaging 4.8
Invest radiol 4.7
Eur Radiol 3.6
MRM 3.3
Int J Cardiovas Imag 2.5
Jul 4, 2011
Solo

Most readers go solo when reading CMR exams. They leave a double reading for complicated cases only.
Jun 23, 2011
Paper of the week
Late gadolinium enhanced cardiovascular magnetic resonance of lamin A/C gene mutation related dilated cardiomyopathy (Journal of Cardiovascular Magnetic Resonance 2011, 13:30 )
Jun 14, 2011
Paper of the week
Sex and Race Differences in Right Ventricular Structure and Function: The Multi-Ethnic Study of Atherosclerosis–Right Ventricle Study (Circulation. 2011;123:2542-2551.)
Right ventricular (RV) morphology is an important predictor of outcomes in heart and lung disease. Dr Kauwt and cols from the John`s Hopkins Hospital examined the demographic factors associated with RV morphology and function in a population-based multiethnic sample free of clinical cardiovascular disease and concluded that age, sex, and race are associated with significant differences in RV mass, RV volumes, and RV ejection fraction, potentially explaining distinct responses of the RV to cardiopulmonary disease.
Jun 5, 2011
Relation of myocardial T2* to right ventricular function in thalassaemia major (EHJ,2010:31, 1648–1654)
Dr. Francisco Alpendurada and cols, supervised by Prof. Dudley Pennell from the Royal Brompton Hospital in London, have many studies about Iron Overload. One very interesting is about RV iron deposition. We can`t miss it... They concluded that myocardial iron deposition is strongly associated with RV dysfunction, which mirrors the decrease in LV function seen with worsening cardiac iron loading. Right ventricular dysfunction may play a significant role in heart failure associated with myocardial siderosis...
Dr. Francisco Alpendurada and cols, supervised by Prof. Dudley Pennell from the Royal Brompton Hospital in London, have many studies about Iron Overload. One very interesting is about RV iron deposition. We can`t miss it... They concluded that myocardial iron deposition is strongly associated with RV dysfunction, which mirrors the decrease in LV function seen with worsening cardiac iron loading. Right ventricular dysfunction may play a significant role in heart failure associated with myocardial siderosis...
Jun 1, 2011
Angiotomografia de coronárias CDI: Início do Blog
Angiotomografia de coronárias CDI: Início do Blog: "Olá a todos, a partir de hoje usaremos esse canal para divulgarmos informações e conhecimento sobre a tomografia de coron..."
May 23, 2011
Atrial fibrilation and CMR
Looks like LGE in atrial fibrillation is not defined protocol standard. Given the limited data on the subject we might not more papers from other groups to really establish the method.
May 21, 2011
Interesting paper:
For those who are interested CMR and in iron overload, Dr. Seldrum and cols recently published that multiple transfused patients with normal ejection fraction and without heart failure have subclinical alterations of systolic and diastolic LV function in direct relation to the severity of cardiac iron overload. Among all parameters, left ventricular twist is affected earliest, and has the highest correlation to log (T2*), suggesting that this parameter might be used to follow systolic left ventricular function in patients with iron overload. http://jcmr-online.com/content/pdf/1532-429x-13-23.pdf (open access).
May 17, 2011
Suggested paper of the week
Cardiac magnetic resonance imaging for the diagnosis of patients presenting with chest pain, raised troponin, and unobstructed coronary arteries (Int J Cardiovasc Imaging. 2011 May 3).
Dr Gerbaud and cols aimed to evaluate the incremental diagnostic and prognostic value of cardiac magnetic resonance (CMR) in 130 patients with chest pain, raised troponin and unobstructed coronary arteries, and to compare subsequent event rates between diagnostic groups. In their study, when a single diagnosis was suspected by the referring physician, CMR validated this diagnosis in 32 patients (76.2%). CMR provided a formal diagnosis in 61 patients (69.3%) in which the clinical diagnosis was uncertain between at least two possibilities. CMR corrected a wrong diagnosis in 10 patients (7.7%). CMR-suggested diagnosis led to a modification of therapy in 42 patients (32.3%). Median follow-up was 34 months in 124 patients. Sixteen patients (12.9%) experienced major adverse cardiovascular events (MACE), but MACE rate was not different between patients with a conclusive CMR and normal CMR. They concluded that in patients with acute troponin-positive chest pain and unobstructed coronary arteries, early CMR has important diagnostic and therapeutic implications. However its association with occurrence of MACE during mid term follow-up was not obvious.
May 7, 2011
SCMR/NHLBI-NIH CMR State of the Art Course
SCMR/NHLBI-NIH CMR State of the Art Course
June 12-13, 2011
Natcher Conference Center
on the NIH Campus
Bethesda, MD
www.scmr.org
Dear colleagues,
The application deadline for a travel grant to attend the SCMR/NHLBI State of the Art CMR Course has been extended until Wednesday, May 11. The lottery drawing for the grants will take place on Friday, May 13!
This two-day introductory, state of the art course on cardiovascular MRI (CMR) is appropriate for those at introductory or intermediate level knowledge of the field. Please forward this information to all colleagues who might be interested in attending.
This course is designed for clinical practitioners, cardiology fellows, radiology residents, technologists/allied health professionals, and will include lectures, case reviews, and interactive workshops by leading faculty in the field.
This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of the Society for Cardiovascular Magnetic Resonance and the University of Minnesota. The University of Minnesota is accredited by the ACCME to provide continuing medical education for physicians.
This activity has been approved for AMA PRA Category 1 credit™. Determination of exact number of credits is pending.
Visit the SCMR website for additional information.
We hope to see you at the course!
David Bluemke, MD, PhD
Gregory Hundley, MD
Christopher Kramer, MD
June 12-13, 2011
Natcher Conference Center
on the NIH Campus
Bethesda, MD
www.scmr.org
Dear colleagues,
The application deadline for a travel grant to attend the SCMR/NHLBI State of the Art CMR Course has been extended until Wednesday, May 11. The lottery drawing for the grants will take place on Friday, May 13!
This two-day introductory, state of the art course on cardiovascular MRI (CMR) is appropriate for those at introductory or intermediate level knowledge of the field. Please forward this information to all colleagues who might be interested in attending.
This course is designed for clinical practitioners, cardiology fellows, radiology residents, technologists/allied health professionals, and will include lectures, case reviews, and interactive workshops by leading faculty in the field.
This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of the Society for Cardiovascular Magnetic Resonance and the University of Minnesota. The University of Minnesota is accredited by the ACCME to provide continuing medical education for physicians.
This activity has been approved for AMA PRA Category 1 credit™. Determination of exact number of credits is pending.
Visit the SCMR website for additional information.
We hope to see you at the course!
David Bluemke, MD, PhD
Gregory Hundley, MD
Christopher Kramer, MD
Suggested paper of the week
Dynamic Changes of Edema and Late Gadolinium Enhancement after Acute Myocardial Infarction and Their Relationship to Functional Recovery and Salvage Index (Circ Cardiovasc Imaging. 2011 Mar 29. [Epub ahead of print])
Dr Erica Dall'Armellina and cols investigated changes in edema and late gadolinium enhancement (LGE) with serial imaging early after acute MI, relating these to global and segmental myocardial function at 6 months. They concluded that myocardial edema is maximal and constant over the first week post MI, providing a stable window for the retrospective evaluation of area at risk. By contrast, myocardial areas with high signal intensity in LGE images recede over time with corresponding recovery of function, indicating that acutely detected LGE does not necessarily equate with irreversible injury and may severely underestimate salvaged myocardium.
May 3, 2011
Suggested paper of the week:
Regional Left Ventricular Myocardial Dysfunction as a Predictor of Incident Cardiovascular Events MESA (Multi-Ethnic Study of Atherosclerosis) J Am Coll Cardiol. 2011 Apr 26;57(17):1735-44
Dr. Yan and his cols from the Johns Hopkins Hospital (USA) examined the prognostic value of subclinical left ventricular (LV) regional myocardial dysfunction (RMD) measured by magnetic resonance imaging (MRI) among asymptomatic individuals in an asymptomatic multiethnic American cohort and concluded that RMD is an independent predictor beyond traditional risk factors and global LV assessment for incident heart failure and atherosclerotic cardiovascular events.
Apr 26, 2011
Looking for NSF

None of the readers reported cases of NSF in the recent years. Small public but very representative. Let's hope it keeps this way.

Original Articles
Regional Thicknesses and Thickening of Compacted and Trabeculated Myocardial Layers of the Normal Left Ventricle Studied by Cardiovascular Magnetic Resonance
Dana K. Dawson, DM, MRCP, DPhil, Alicia M. Maceira, MD, Vimal J. Raj, MB, BS, FRCR, Catriona Graham, MSc, BSc(hons), Dudley J. Pennell, MD, FRCP, FACC, FESC and Philip J. Kilner, MD, PhD
Abstract
Background— We used cardiovascular magnetic resonance (CMR) to study normal left ventricular (LV) trabeculation as a basis for differentiation from pathological noncompaction.
Methods and Results— The apparent end-diastolic (ED) and end-systolic (ES) thicknesses and thickening of trabeculated and compacted myocardial layers were measured in 120 volunteers using a consistent selection of basal, mid, and apical CMR short-axis slices. All had a visible trabeculated layer in 1 or more segments. The compacted but not the trabeculated layer was thicker in men than in women (P<0.01 at ED and ES). When plotted against age, the trabeculated and compacted layer thicknesses demonstrated opposite changes: an increase of the compact layer after the fourth decade at both ED and ES (P<0.05) but a decrease of the trabeculated layer. There was age-related preservation of total wall thickness at ED but an increase at ES (P<0.05). The compacted layer thickened, whereas the trabeculated layer thinned with systole, but neither change differed between sexes. With age, the most trabeculated LV segments showed significantly greater systolic thinning of trabeculated layers and, conversely, greater thickening of the compact segments (P<0.05). Total wall thickening is neither sex nor age dependent. There were no sex differences in the trabeculated/compacted ratio at ES or ED, but the ES trabeculated/compacted ratio was smaller in older (50 to 79 years) versus younger (20 to 49 years) groups (P<0.05).
Conclusions— We demonstrated age- and sex-related morphometric differences in the apparent trabeculated and compacted layer thicknesses and systolic thinning of the visible trabeculated layer that contrasts with compacted myocardial wall thickening.
Key Words:myocardiumtrabeculae, myocardium, systolic thickeningisolated noncompaction of the ventricular myocardiumcontractility.
© 2011 American Heart Association, Inc.

Cardiac Magnetic Resonance of Left Ventricular Trabeculation
The New Normal
Elizabeth M. McNally, MD, PhD and Amit R. Patel, MD
Key Words:Editorial sheart ventricle isolated noncompaction of the ventricular myocardium cardiomyopathy magnetic resonance imaging .Historically, left ventricular noncompaction (LVNC) was considered to be a rare form of cardiomyopathy; however, during the past decade, there has been a significant increase in reports of patients with LVNC. Using either echocardiography or cardiac magnetic resonance (CMR) imaging, LVNC is relatively straight forward to diagnose in individuals expressing a typical phenotype. However, the diagnosis may be challenging to make in those individuals who express more subtle phenotypes of LVNC. CMR imaging offers a more detailed examination of myocardial structure and composition compared with other imaging modalities, such as echocardiography. With more common use of CMR, there has been increased appreciation of the degree of trabeculation of the LV. The ventricle comprises 2 myocardial layers: the compact myocardium and the trabecular myocardium. During cardiac development, after heart looping, the myocardium becomes deeply trabeculated through a clonal outgrowth of embryonic cardiomyocytes. 1 After the coronary arteries form and provide a ready supply of oxygen and nutrients, the LV undergoes compaction accompanied by resolution of the deep trabeculae. Persistence of the LV trabeculae in the postnatal myocardium may be associated with cardiomyopathy, and LVNC is classified as a cardiomyopathy. 2, 3
Circulation: Cardiovascular Imaging.2011; 4: 84-86
Apr 24, 2011
Suggested Paper of the week: On T2* Magnetic Resonance and Cardiac Iron
Dr. John-Paul Carpenter's and cols recent publication is about measurement of myocardial iron, that is key to the clinical management of patients at risk of iron-overload cardiomyopathy, which is a major killer in transfusion-dependent patients and others with errors of iron metabolism. They observed a strong correlation between cardiovascular magnetic resonance relaxation measurements and biochemically derived tissue iron concentration in 12 postmortem human hearts from transfusion-dependent patients, leading to a clinical calibration equation.
Apr 18, 2011
The Extent of Left Ventricular Scar Quantified by Late Gadolinium Enhancement MRI Is Associated with Spontaneous Ventricular Arrhythmias in Patients with Coronary Artery Disease and Implantable Cardioverter Defibrillators.
This pilot study from Dr. Scott et al, suggested that the extent of myocardial scar, characterised by LGE-CMR, was significantly associated with the occurrence of spontaneous ventricular arrhythmias. Their hypothesis is that scar quantification by LGE-CMR may prove a valuable risk stratification tool for the occurrence of ventricular arrhythmias, which may have implications for patient selection for ICD therapy.
Apr 12, 2011
Incremental Prognostic Significance of Combined Cardiac Magnetic Resonance Imaging, Adenosine Stress Perfusion, Delayed Enhancement, and Left Ventricular Function Over Preimaging Information for the Prediction of Adverse Events
(Circulation. 2011;123:1509-1518.)
Dr. Binghan and Dr. Hachamovitch followed 908 patients with suspicion of coronary stenosis and/or ischemia and concluded that CMR analysis of ventricular volume, aortic flow, myocardial viability, and stress perfusion all add incremental value for prediction of adverse events over pre-CMR data and can be combined to further enhance prognostication. Normal combined CMR confers a low risk of subsequent cardiac events.
Apr 1, 2011
Every CMR information is important

An early release from Circulation shows that every bit of information on CMR assessment of ischemic patients is relevant and adds prognostic data to pre-imaging parameters.
http://www.blogger.com/img/blank.gif
http://circ.ahajournals.org - online first
Mar 31, 2011
Reporting Live from Brasilia - Brazilian Cardiovascular Imaging Meeting

Brazilian Society of Cardiology was one of the first in the world to unify all its imaging groups into a single Imaging Department. This has led to an annual Imaging Department Meeting, which is now on its third edition. More than 1000 participants from the country and LatAm are present with these year's lectures being much more interactive and multi-modality focused.
More information on: http://www.congressodepeco.com.br/
Tablets not so widespread in CMR

Half of the responders use tablets on daily practice. Still some ground to catch on and see the real application of these devices in CMR.
Mar 20, 2011
LGE in Endomyocardial Fibrosis Patients
Salemi et al from Heart Institute in Brazil just published a new manuscript assessing the diagnosis and prognosis of LGE in EMF in Circ Imaging. Congratulations on the group which has been very active in the last years in LatAm.
Salemi VM. Circ Cardiovasc Imaging. 2011 Mar 17. [Epub ahead of print] - Link here.
Salemi VM. Circ Cardiovasc Imaging. 2011 Mar 17. [Epub ahead of print] - Link here.
Mar 16, 2011
7T in vivo and ECG triggering

Brandts et al compared LV function analysis using 7T to the gold standard 1.5T. While the results were comparable, 20% of patients did not complete the exam due to ECG triggering problem. While this shows the potential of 7T it is rather bothersome to find 20% of failure rates, leading to the conclusion that new forms of gating will have to be developed if we are to go further than 3T.
Link here. Brandts A et al. MRM 2010;64:1471-7.
Mar 13, 2011
J Am Coll Cardiol Img, 2011
Evaluation of Techniques for the Quantification of Myocardial Scar of Differing Etiology Using Cardiac Magnetic Resonance
Objectives: The aim of this study was to compare the reproducibility of 7 late gadolinium enhancement (LGE) quantification techniques across 3 conditions in which LGE is known to be important: acute myocardial infarction (AMI), chronic myocardial infarction (CMI), and hypertrophic cardiomyopathy (HCM).
Background: LGE by cardiac magnetic resonance is the gold-standard technique for assessing myocardial scar. No consensus exists on the best method for its quantification, and research in this area is scant. Techniques include manual quantification, thresholding by 2, 3, 4, 5, or 6 SDs above remote myocardium, and the full width at half maximum (FWHM) technique. To date, LGE has been linked to outcome in 3 conditions: AMI, CMI, and HCM.
Methods: Sixty patients with 3 LGE etiologies (AMI, n = 20; CMI, n = 20; HCM, n = 20) were scanned for LGE. LGE volume was quantified using the 7 techniques. Mean LGE volume, interobserver and intraobserver reproducibility, and impact on sample size were assessed.
Results: LGE volume varied significantly with the quantification method used. There was no statistically significant difference between LGE volume by the FWHM, manual, and 6-SD or 5-SD techniques. The 2-SD technique generated LGE volumes up to 2 times higher than the FWHM, 6-SD, and manual techniques. The reproducibility of all techniques was worse in HCM than AMI or CMI. The FWHM technique was the most reproducible in all 3 conditions compared with any other method (p < 0.001). Use of the FWHM technique for LGE quantification in paired analysis would lead to at least a 60% reduction in required sample size compared with any other method.
Conclusions: Regardless of the disease under study, the FWHM technique for LGE quantification gives LGE volume mean results similar to manual quantification and is statistically the most reproducible, reducing required sample sizes by up to one-half.
Key Words: cardiac magnetic resonance • cardiomyopathy • imaging • myocardial infarction • SVCs
Evaluation of Techniques for the Quantification of Myocardial Scar of Differing Etiology Using Cardiac Magnetic Resonance
Objectives: The aim of this study was to compare the reproducibility of 7 late gadolinium enhancement (LGE) quantification techniques across 3 conditions in which LGE is known to be important: acute myocardial infarction (AMI), chronic myocardial infarction (CMI), and hypertrophic cardiomyopathy (HCM).
Background: LGE by cardiac magnetic resonance is the gold-standard technique for assessing myocardial scar. No consensus exists on the best method for its quantification, and research in this area is scant. Techniques include manual quantification, thresholding by 2, 3, 4, 5, or 6 SDs above remote myocardium, and the full width at half maximum (FWHM) technique. To date, LGE has been linked to outcome in 3 conditions: AMI, CMI, and HCM.
Methods: Sixty patients with 3 LGE etiologies (AMI, n = 20; CMI, n = 20; HCM, n = 20) were scanned for LGE. LGE volume was quantified using the 7 techniques. Mean LGE volume, interobserver and intraobserver reproducibility, and impact on sample size were assessed.
Results: LGE volume varied significantly with the quantification method used. There was no statistically significant difference between LGE volume by the FWHM, manual, and 6-SD or 5-SD techniques. The 2-SD technique generated LGE volumes up to 2 times higher than the FWHM, 6-SD, and manual techniques. The reproducibility of all techniques was worse in HCM than AMI or CMI. The FWHM technique was the most reproducible in all 3 conditions compared with any other method (p < 0.001). Use of the FWHM technique for LGE quantification in paired analysis would lead to at least a 60% reduction in required sample size compared with any other method.
Conclusions: Regardless of the disease under study, the FWHM technique for LGE quantification gives LGE volume mean results similar to manual quantification and is statistically the most reproducible, reducing required sample sizes by up to one-half.
Key Words: cardiac magnetic resonance • cardiomyopathy • imaging • myocardial infarction • SVCs
Mar 8, 2011
SCMR-LAC Ballot Info

This year we have to renew some positions in the SCMR Latin American Chapter. It is very important to get new people involved and to get fresh ideas onboard.
Positions for the 2011-2013 Latin American Working Group
1. Chair: represent the LAC inside SCMR; organize the other positions to keep focused goals; write a formal column in the newsletter;
2. Newsletter editor(s): write and/or organize the text for the LAC Newsletter every 3 months (4 editions/year – 2 pages); does not need to hard print the newsletter but provide it with content mostly.
3. Webpage/twitter editor(s): be responsible for at least weekly updates on both channels of communication for the LAC
4. Financial coordinator(s): as all know, the LAC has only raised funds for some of its meetings; however, with the webpage and newsletter and the over 100 physicians that follow the group we find that there are opportunities to gain some local funding from LatAm based companies.
5. Meeting coordinator(s): responsible to seek opportunities and organize with the host country local organizer the LAC meetings. The focus of the meetings is mainly to foster the use of CMR in the country which the meeting is hosted, usually within or together with a major cardiology/radiology meeting of the host country. The task is to find this country every year and work with the local committee to help the meeting take place yearly.
If you are a SCMR member or want to join SCMR and participate please let us know. You are allowed to join SCMR until March 31 to be eligible.
How the voting process will occur:
1. Candidates should send their names, position to be voted for and a 3-10 line mini-CV to jlaraf@fcm.unicamp.br until March 31 (Thursday)
2. All candidates will be checked for eligibility – if they are SCMR members or have just joined SCMR at this time.
3. All nominations will be announced on April 4 (Monday) and sent to SCMR Headquarters.
4. The ballot will be handled centrally to avoid any biases by SCMR Headquarters and will start one week after the announcement of the nominations
5. SCMR Latin American members will vote on the candidates for a period of 15 days
6. The new positions will be announced on April 19.
Please note that you can be candidate for more than one position and that some positions will accept more than one person.
Thanks in advance and feel free to write if you have any doubts. Please check the website to get more acquainted to our activities.
Juliano Lara Fernandes, MD, PhD
University of Campinas (Unicamp) - Brazil
Mar 6, 2011
T2 imaging - not so easy

According to readers of the blog, getting the sequences to work are not so straightforward suggesting more work is needed.
Feb 27, 2011
New Latin American Cardiac Imaging Site

Started this week - promises to be very educational.
Content initially in Portuguese.
Many thanks to Marcelo Hadlich and Rochelle Coppo.
http://www.imagemcardiologica.com.br/
Feb 26, 2011
CMR Perfusion - gold standard

This was news on Auntminnie. I quote:
"Dynamic cardiac CT stress perfusion equivalent to MRI
By Eric Barnes, AuntMinnie.com staff writer
Cardiac MRI may be the gold standard for evaluating myocardial perfusion, but there's no reason CT can't eventually take over much of MRI's workload in patients suspected of coronary artery disease"
OK, it's a site dedicated to imaging but it is very good news to hear that CMR is being considered as the gold standard for perfusion. Very stimulating!
Feb 22, 2011
T2 review - more debate

A new review on T2 imaging was recently launched in JCMR.
Read the free full text at: http://jcmr-online.com/content/pdf/1532-429X-13-13.pdf
The debate is on!
Feb 17, 2011

Feb 10, 2011
What was hot in SCMR 2011

Our votes indicated that T2 and edema imaging would be hot. Well, it was in a way but a lot of controversy arose this year. More robust data was demanded from many speakers and certainly new data will have to be put forward to put this powerful tool into real clinical setting.
Jan 31, 2011
LGE and fibrosis: spread the word

A comprehensive review targeted at physicians of LGE and myocardial fibrosis:
Non-invasive evaluation of myocardial fibrosis:implications for the clinician
Darryl P Leong, Per Lav Madsen and Joseph B Selvanayagam
Heart 2010 96: 2016-2024
Link here.
Pharmacointesive versus primary PCI by CMR

An interesting study using CMR endpoints (infarct size, salvaged myocardium, microvascular obstruction, volumes and ejection fraction) by Bodí et al from Spain to assess whether any differences were observed between primary PCI and a pharmacointensive strategy in the treament of STEMI. No differences were observed among the strategies as was very clearly shown by CMR.
Full text in Spanish and English at: http://www.revespcardiol.org/ficheros/eop/S0300-8932%2810%2900047-3.pdf - Online First
Jan 24, 2011
Two Latin American events in SCMR/EuroCMR 2011

There are two specific events for Latin American participants during this year's sessions:
Saturday
07:00 to 08:00 – Latin American WG – Galliéni 2
Sunday
07:00 to 08:00 – Case Review Session – Mixed Cases from Latin America – Room Risso
Both at 07:00, so be early! Tips for waking up early on http://www.howtowakeupearly.com/

Jan 19, 2011
Look into the aorta
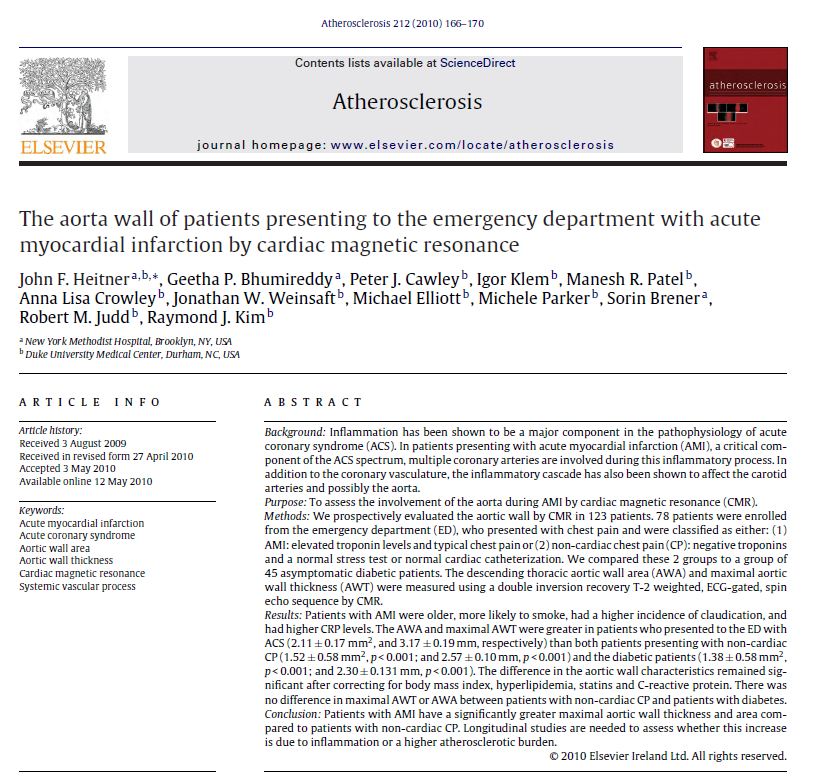
A simple double IR FSE sequence in mid thorax can help a lot in identifying patients with increased risk of events as shown by Heitner JF et al in Atherosclerosis. Greater aortic wall thickness and area seems to give a lot of information compared to controls and DM patients.
Link here.
Jan 18, 2011
Going to Nice

Let's see if the number of LatAm attendees increase compared to next year. Half of the respondents are planning to go:
Jan 11, 2011
Do you want to train your techs in CMR?

Two video lessons (in Portuguese) were recorded by Dr Carlos Rochitte (InCor - University of Sao Paulo and HCor-SP) and are available for download (please see useful links on the left).
The lessons are very comprehensive and provide a complete training program for MR techs interested in learning or updating in CMR.
Link in http://gallery.me.com/rochitte

Jan 3, 2011

Subscribe to:
Comments (Atom)
